Breast surgery
Adnexa surgery
Uterine surgery
Cervical surgery
Vulvar surgery
Other
Pelvic Organ Prolapse (POP)
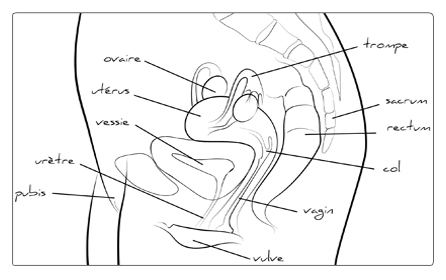
The Pelvic Organ Prolapse is the abnormal descent or herniation of the pelvic organs from their normal attachment sites or their normal position in the pelvis. The pelvic structure that may be involved include the uterus (uterine prolapse) or vaginal apex (apical vaginal prolapse), anterior vagina (cystocele), or posterior vagina (rectocele). When nonsurgical procedures failed, some other treatments may be considered, in order to position the prolapsed organs back and to fix them to the pelvic floor.
For the 3 surgical procedures, a general anaesthesia or a regional one (epidural block or spinal anaesthesia) is administrated.
Procedures available to treat POP:
Vaginal approach
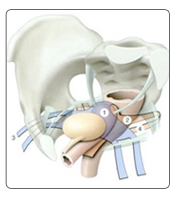
The surgery is performed transvaginally and excludes any abdominal incision. Usually the uterus is removed. It consists by mooring the uterus or the top of the vagina (if the uterus is removed) to ligaments of the pelvic floor. If the bladder and/or the rectum go down, they need to be supported:
- whether by using the natural ligaments and muscles
- whether by using synthetic strips or prostheses, as with the TVM technic (Tension-free Vaginal Mesh).
Prostheses used are made of Prolene or Polypropylene. This is a synthetic non-absorbable, flexible fabric and especially designed to be placed in the pelvis and to support the prolapsed organs. Its advantages include minimal tissue reactivity as well as durability. While performing small incisions, the surgeon will place this prosthesis through the top of the vagina in order to reinforce the support tissues and to replace the organs in their anatomical position. The intervention lasts approximately 60 minutes, which is shorter than the traditional technics. Moreover this new method preserves the uterus when it is not bad, and an urinary incontinence treatment is possible at the same time. The hospital stay is around 3 days, and the work leave is 15 days.

Abdominal Approach through laparotomy
The procedure may be performed by an open laparotomy (abdominal incision) approach. The uterus is either preserved or removed. The vagina or the uterus, the bladder and the rectum will be fixed in place with the help of grafts and sutures onto a solid element of the pelvis. The hospital stay is approximately 6 days long, and the work leave is 1 month.
Abdominal Approach through laparoscopic
This procedure is most likely performed than the laparotomy one. A lighted laparoscope, camera and small instruments are inserted through tiny incisions in the abdomen (umbilicus). Prolapsed organs will then be fixed back to their anatomical place with prostheses or sutures onto a solid element of the pelvis, as it is performed through laparotomy. You will remain at the hospital for a maximum of 3 days, and the sick leave is 15 days long.
Risks & Complications
Even if surgery procedures and technics are meticulous, it is not possible to guarantee neither therapeutic success nor a complete absence of intraoperative complications.
During the intervention
- The abdominal incision: the access incision can be modified (“laparoconversion”, i.e. from a laparoscopic to a laparotomy one) according to the observations made during the operation, or if any per-operational complications occurred.
- Significant blood loss: may rarely lead to a blood transfusion
- Lesions of an organ close to the uterus: this can exceptionally happen: intestinal, urinary tracts or blood vessels wounds, requiring a specific surgical assumption.
Post-operation
- Blood tumor or abscess in the abdominal wall: it generally requires local care, but a surgical evacuation may be an option.
- Lower extremity deep venous thrombosis and pulmonary embolism: in order to prevent this kind of complication, an early rising is recommended, as well as wearing support stockings and daily injections of anticoagulant.
- Bowel obstruction: It can require a medical care, even a surgical operation.
- Healing failings with the prosthesis: vaginal tissues healing process is aborted by the presence of the grafts or meshes used to repair. A simple surgery is needed, to remove the visible part of the prosthesis.
- The retraction of the prosthesis: responsible of pelvic pains or pains during sexual intercourses. If the retraction is too important, a partial or total section of it one can be necessary
Last update: 10/2/2013